
1. Introduction: The Body’s Master Chemist
The kidneys are among the most quietly sophisticated organs in the human body. Roughly the size of a clenched fist and shaped like the bean that bears their name, this pair of organs filters the entire blood volume of the body around forty times every day. They are not merely passive sieves that strain waste from blood; they are dynamic, computational chemical processors that make second-by-second decisions about what the body keeps and what it discards.
To call the kidney a filter understates it profoundly. A coffee filter cannot decide to retain sugar while rejecting urea, nor can it sense that the blood has become too acidic and respond by manufacturing new bicarbonate. The kidney does all of this and more. It governs the volume and pressure of the circulation, the concentration of every major ion, the acidity of the internal environment, the production of red blood cells, the activation of vitamin D, and the long-term regulation of blood pressure.
Central thesis of this articleThe kidney is best understood not as a waste-disposal organ but as the body’s principal homeostatic regulator — the organ that defines and defends the chemical composition of the internal environment within which every other cell must live.
This document examines the kidney from the ground up. It begins with gross anatomy, descends to the microscopic functional unit — the nephron — and then to the molecular machinery embedded in nephron cell membranes. From this structural foundation it builds an account of the four core processes of urine formation, the detailed handling of each major electrolyte, the regulation of acid–base balance and water, and finally the kidney’s endocrine roles and what happens when the system fails.
2. Gross Anatomy and Position
The two kidneys are retroperitoneal organs, meaning they sit behind the peritoneal membrane that lines the abdominal cavity, against the posterior abdominal wall. In an adult, each kidney measures approximately 10 to 12 centimetres in length, 5 to 7 centimetres in width, and around 3 centimetres in thickness, weighing between 120 and 170 grams. The right kidney typically sits slightly lower than the left because the liver occupies space above it.
2.1 External and Internal Structure
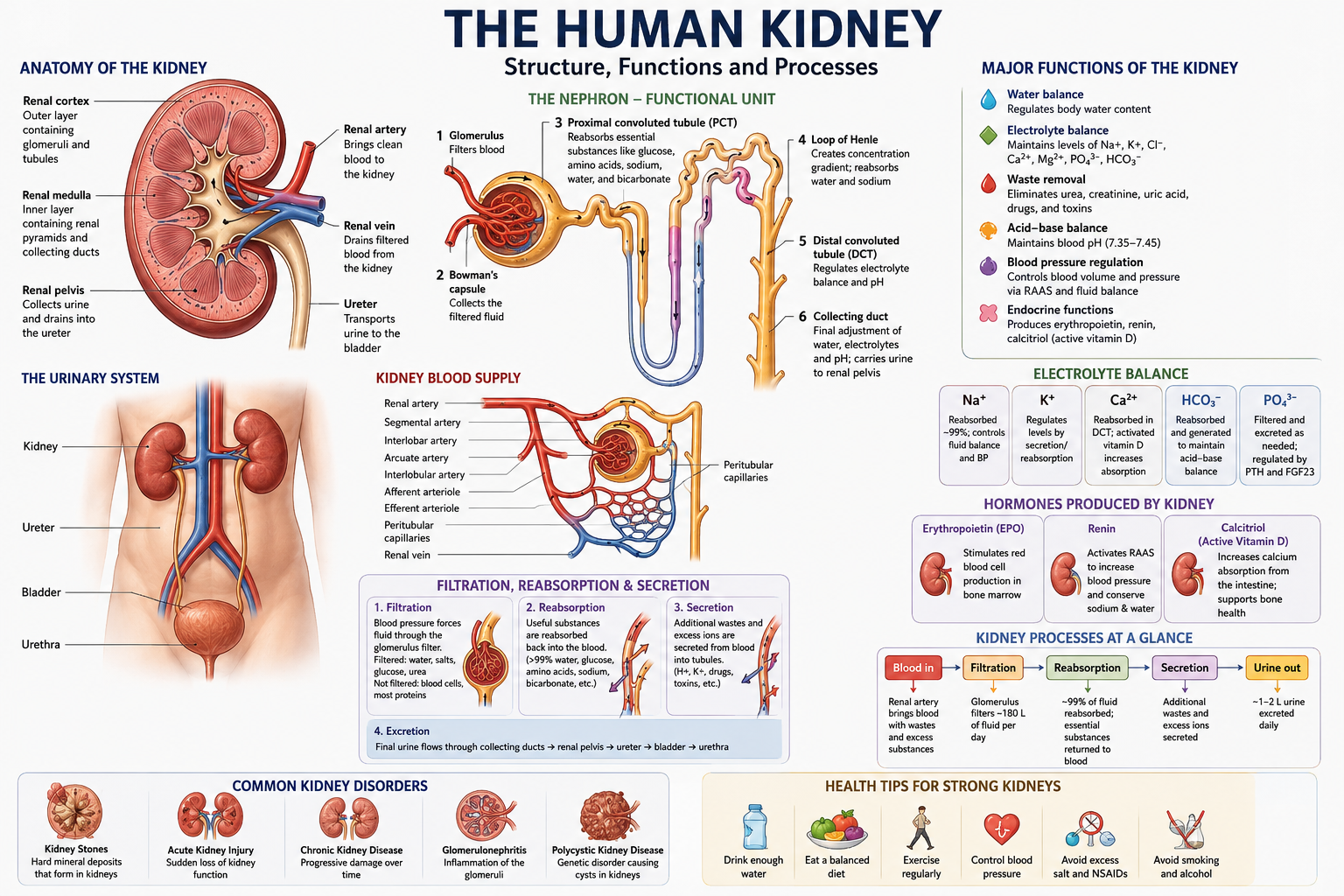
Each kidney is wrapped in three protective layers: an inner fibrous capsule that adheres directly to the organ surface, a middle cushion of perirenal fat, and an outer renal fascia that anchors the kidney in place. The concave medial border features the hilum, a slit through which the renal artery enters and the renal vein and ureter exit.
Cutting a kidney lengthwise reveals two clearly distinct regions. The outer renal cortex is granular and reddish-brown. The inner renal medulla is organised into 8 to 18 cone-shaped renal pyramids, whose tips (the renal papillae) point inward toward the collecting spaces. Urine drips from the papillae into cup-shaped minor calyces, which merge into major calyces, which in turn empty into the funnel-like renal pelvis that becomes the ureter.
| Structure | Location | Primary role |
|---|---|---|
| Renal cortex | Outer region | Contains glomeruli and most tubule segments |
| Renal medulla | Inner region | Contains loops of Henle and collecting ducts; concentrates urine |
| Renal pyramids | Within medulla | Cone-shaped functional bundles draining to papillae |
| Renal papilla | Pyramid tip | Releases formed urine into minor calyx |
| Calyces & pelvis | Central sinus | Collect and channel urine toward the ureter |
| Hilum | Medial border | Entry/exit for vessels, nerves, and ureter |
2.2 Blood Supply: A Privileged Circulation
The kidneys receive a strikingly disproportionate share of the cardiac output. Although together they account for less than half a percent of body weight, they receive roughly 20 to 25 percent of the blood the heart pumps at rest — about 1.2 litres of blood per minute. This enormous perfusion reflects the kidney’s role: it must continually sample and reprocess the entire bloodstream.
Blood enters through the renal artery, which branches successively into segmental, interlobar, arcuate, and cortical radiate arteries, finally giving rise to the afferent arterioles. Each afferent arteriole feeds a tuft of capillaries called the glomerulus. Crucially, blood leaves the glomerulus not through a vein but through a second arteriole — the efferent arteriole — an arrangement found almost nowhere else in the body. This two-arteriole design lets the kidney independently regulate the pressure inside the glomerular capillaries, which is the engine of filtration.
Why two arterioles matterBy constricting or dilating the afferent (incoming) and efferent (outgoing) arterioles independently, the kidney can fine-tune glomerular pressure and thus filtration rate even when systemic blood pressure swings — a capacity called autoregulation.
3. The Nephron: The Functional Building Block
If anatomy gives the kidney its shape, the nephron gives it its function. Each kidney contains roughly one million nephrons, and these microscopic units are where every act of filtration, reabsorption, secretion, and concentration actually occurs. A kidney is, in essence, a million tiny kidneys working in parallel. Importantly, nephrons cannot regenerate; the number a person is born with declines gradually across life, which is why kidney reserve matters so much in ageing and disease.
3.1 The Two Major Components
A nephron has two functionally linked parts. The renal corpuscle is the filtering apparatus, and the renal tubule is the long, winding pipe that processes the filtrate into urine. The renal corpuscle itself consists of the glomerulus (the capillary tuft) and the surrounding Bowman’s capsule, a double-walled cup that captures the fluid pushed out of the capillaries.
3.2 The Anatomical Journey of Filtrate
Fluid filtered into Bowman’s capsule travels through a precisely ordered sequence of tubule segments, each with a distinct cellular character and transport job:
- Proximal convoluted tubule (PCT): the workhorse of reabsorption, lined with cells bearing a dense brush border of microvilli that vastly expand surface area.
- Loop of Henle: a hairpin that dives into the medulla and returns, comprising a thin descending limb, a thin ascending limb, and a thick ascending limb. It establishes the concentration gradient that makes water conservation possible.
- Distal convoluted tubule (DCT): a shorter segment specialised for fine-tuned, hormonally controlled adjustment of sodium, calcium, and acid balance.
- Collecting duct: the final common pathway where multiple nephrons converge; the principal site of hormone-controlled water and potassium regulation before urine leaves the kidney.
3.3 Cortical and Juxtamedullary Nephrons
Not all nephrons are alike. About 85 percent are cortical nephrons, with short loops that barely penetrate the medulla; these handle the bulk of routine reabsorption. The remaining 15 percent are juxtamedullary nephrons, whose long loops plunge deep into the medulla. These long-looped nephrons, paired with specialised straight capillaries called the vasa recta, are responsible for the kidney’s remarkable ability to produce concentrated urine and conserve water during dehydration.
| Feature | Cortical nephron | Juxtamedullary nephron |
|---|---|---|
| Proportion | ~85% | ~15% |
| Loop length | Short | Long, deep into medulla |
| Main role | Routine solute reabsorption | Urine concentration / water conservation |
| Capillary partner | Peritubular capillaries | Vasa recta |
4. Molecular Building Blocks of Filtration
Filtration is not indiscriminate. The glomerular filtration barrier is a three-layered structure exquisitely tuned to size and electrical charge, allowing water and small solutes through while retaining blood cells and large proteins. Understanding these layers explains both how the kidney works and how it fails in disease.
4.1 The Three Filtration Layers
- Fenestrated endothelium: the capillary wall itself is perforated with pores (fenestrae) about 70–100 nanometres wide, blocking blood cells but freely passing plasma.
- Glomerular basement membrane (GBM): a thick gel of collagen IV, laminin, and negatively charged heparan sulphate proteoglycans. Its negative charge repels negatively charged plasma proteins such as albumin.
- Podocyte filtration slits: specialised epithelial cells called podocytes wrap the capillaries in interlocking foot processes (pedicels). The narrow gaps between them are bridged by a protein mesh — the slit diaphragm, built from nephrin and podocin — forming the final and most selective sieve.
Clinical linkWhen podocytes are injured — as in many forms of glomerular disease — the slit diaphragm fails and protein leaks into the urine (proteinuria). Persistent albumin in the urine is one of the earliest and most important warning signs of kidney damage.
4.2 What Passes and What Stays
The filtrate that enters Bowman’s capsule is essentially blood plasma minus its proteins and cells. Water, glucose, amino acids, ions, urea, and other small molecules cross freely. Albumin and larger proteins are held back, both because of their size and because of their negative charge. The result is an ultrafiltrate that the tubules then reshape into urine.
| Component | Freely filtered? | Reason |
|---|---|---|
| Water | Yes | Small, uncharged |
| Sodium, potassium, chloride | Yes | Small ions |
| Glucose & amino acids | Yes | Small; later fully reabsorbed |
| Urea & creatinine | Yes | Small waste molecules |
| Albumin | Largely no | Large and negatively charged |
| Red & white blood cells | No | Far too large for fenestrae |
5. The Four Core Processes of Urine Formation
Urine is produced through four integrated processes. The first three are the classical sequence; the fourth — water handling — is woven through the others but deserves separate treatment because of its importance.
5.1 Glomerular Filtration
Filtration is driven by pressure. Blood pressure inside the glomerular capillaries (around 55 mmHg) pushes fluid outward, opposed by the pressure of fluid already in Bowman’s capsule (about 15 mmHg) and by the osmotic pull of plasma proteins left behind (about 30 mmHg). The net filtration pressure of roughly 10 mmHg drives plasma across the barrier. The total volume filtered per minute is the glomerular filtration rate (GFR), normally about 120 millilitres per minute, or some 180 litres per day — far more than the body’s entire plasma volume, which is why nearly all of it must be reabsorbed.
GFR as the master measure of kidney healthBecause GFR reflects the total filtering capacity of all functioning nephrons, it is the single most important number in clinical kidney medicine. Estimated GFR (eGFR), calculated from blood creatinine, is the standard for staging chronic kidney disease.
5.2 Tubular Reabsorption
Of the 180 litres filtered daily, only about 1.5 litres leave the body as urine. The remaining 99 percent — along with all the glucose, amino acids, and most of the ions — is reclaimed by tubular reabsorption. This recovery is selective and largely active, costing the kidney substantial energy. The proximal convoluted tubule alone reclaims around two-thirds of filtered sodium and water, all of the filtered glucose and amino acids, and most bicarbonate.
5.3 Tubular Secretion
Secretion is reabsorption in reverse: substances move from the peritubular blood into the tubular fluid, adding to what will be excreted. This pathway disposes of hydrogen ions, potassium, ammonia, and many drugs and toxins (including penicillin and metabolic acids). Secretion is also the kidney’s fast lever for adjusting blood pH and potassium.
5.4 Water Handling and Concentration
Water follows solute osmotically, but the kidney can decouple the two to either conserve or shed water. This is achieved through the countercurrent multiplier of the loop of Henle and the hormone-controlled water permeability of the collecting duct, discussed in detail in Sections 7 and 8.
| Process | Direction | Main location | Result |
|---|---|---|---|
| Filtration | Blood → tubule | Glomerulus | Forms protein-free ultrafiltrate |
| Reabsorption | Tubule → blood | Mostly PCT | Recovers water & useful solutes |
| Secretion | Blood → tubule | DCT & collecting duct | Removes H⁺, K⁺, drugs |
| Concentration | Water movement | Loop & collecting duct | Sets final urine volume |
6. Electrolyte Processing in Detail
Electrolytes are the charged ions whose concentrations the kidney guards with extraordinary precision, because nerves, muscles, and the heart all depend on them. Even small deviations in potassium, for example, can be fatal. This section follows each major electrolyte through the nephron.
6.1 Sodium (Na⁺): The Central Currency
Sodium is the dominant extracellular ion and the master regulator of body fluid volume — wherever sodium goes, water tends to follow. The kidney filters around 25,000 millimoles of sodium per day and reabsorbs more than 99 percent of it. The energy for nearly all sodium reabsorption comes from the sodium-potassium ATPase pump on the basolateral (blood-facing) side of tubule cells, which continually pumps sodium out into the blood, keeping intracellular sodium low so that sodium flows in from the tubule down its gradient.
- Proximal tubule (~65%): reabsorbed alongside glucose, amino acids, and bicarbonate via cotransporters and the sodium–hydrogen exchanger.
- Thick ascending limb (~25%): reclaimed by the NKCC2 cotransporter (sodium, potassium, two chlorides) — the target of powerful loop diuretics such as furosemide.
- Distal tubule (~5%): via the sodium–chloride cotransporter (NCC), the target of thiazide diuretics.
- Collecting duct (~3%): through ENaC channels under the control of the hormone aldosterone — the final, finely tuned adjustment.
6.2 Potassium (K⁺): The Tightly Guarded Ion
Potassium is the dominant intracellular ion, and the gap between its high concentration inside cells and low concentration outside sets the resting electrical state of every excitable cell. The kidney both reabsorbs potassium (mostly in the proximal tubule and loop) and secretes it (in the distal tubule and collecting duct). Crucially, it is the regulated secretion in the collecting duct — driven by aldosterone — that matches potassium excretion to intake, protecting the heart from dangerous swings.
A delicate balanceHigh blood potassium (hyperkalaemia) and low blood potassium (hypokalaemia) are both medical emergencies that disturb heart rhythm. The kidney’s distal potassium secretion is the body’s primary defence on both fronts.
6.3 Chloride (Cl⁻), Calcium (Ca²⁺), and Phosphate
Chloride, the principal extracellular anion, is largely reabsorbed alongside sodium, both passively (following sodium’s electrical pull) and actively (via the NKCC2 and NCC cotransporters). Calcium reabsorption is split between passive proximal recovery and tightly regulated distal recovery controlled by parathyroid hormone (PTH). Phosphate handling occurs mainly in the proximal tubule and is likewise restrained by PTH, which reduces phosphate reabsorption to lower blood phosphate when needed.
6.4 Magnesium and Bicarbonate
Magnesium, essential for hundreds of enzymes, is unusual in being reabsorbed largely in the thick ascending limb rather than the proximal tubule. Bicarbonate, the body’s main pH buffer, is almost entirely reabsorbed in the proximal tubule, where it is reclaimed indirectly through hydrogen-ion secretion and the enzyme carbonic anhydrase — a process examined in the acid–base section.
| Electrolyte | Main reabsorption site | Key regulator / transporter |
|---|---|---|
| Sodium (Na⁺) | Proximal tubule + all segments | Na⁺/K⁺-ATPase; aldosterone (ENaC) |
| Potassium (K⁺) | Secreted in collecting duct | Aldosterone |
| Chloride (Cl⁻) | Follows sodium throughout | NKCC2, NCC, passive gradient |
| Calcium (Ca²⁺) | Proximal + distal tubule | Parathyroid hormone (PTH) |
| Phosphate | Proximal tubule | PTH (inhibits reabsorption) |
| Magnesium (Mg²⁺) | Thick ascending limb | Passive, paracellular |
| Bicarbonate (HCO₃⁻) | Proximal tubule | Carbonic anhydrase, H⁺ secretion |
7. Water Balance and the Countercurrent Mechanism
The kidney’s ability to produce urine far more concentrated than blood — or far more dilute — is one of its most elegant feats. It rests on a structural arrangement called the countercurrent multiplier, located in the loop of Henle of the long juxtamedullary nephrons.
7.1 Building the Medullary Gradient
The two limbs of the loop of Henle have opposite permeabilities. The descending limb is permeable to water but not to salt, so water leaves and the fluid inside grows concentrated as it descends. The ascending limb is impermeable to water but actively pumps out salt, so the fluid grows dilute as it rises. Because the two limbs run side by side in opposite directions, the salt pumped out of the ascending limb raises the concentration around the descending limb, which loses still more water — a self-reinforcing loop that multiplies a modest gradient into a steep one, making the deep medulla extremely salty.
7.2 The Vasa Recta and Urea Recycling
The medullary gradient would be washed away by ordinary blood flow, so the vasa recta — hairpin capillaries that parallel the loop — act as countercurrent exchangers, removing reabsorbed water without dissipating the salt gradient. Urea also contributes: recycled between the collecting duct and the medullary interstitium, it accounts for a large share of the deep medulla’s osmotic pull, adding to the kidney’s concentrating power.
7.3 Cashing In the Gradient
This steep medullary gradient is the prize. As urine flows through the collecting duct, which passes back down through the salty medulla, water can be drawn out osmotically — but only if the duct is permeable to water. Whether it is depends on a single hormone, antidiuretic hormone, which forms the bridge to the next section.
8. Hormonal Control of Kidney Function
The kidney is both a target of hormones and a producer of them. Three hormonal systems dominate the regulation of fluid, electrolytes, and blood pressure.
8.1 Antidiuretic Hormone (ADH / Vasopressin)
Released from the posterior pituitary when the blood becomes too concentrated or blood volume falls, ADH acts on the collecting duct. It instructs duct cells to insert water channels called aquaporin-2 into their membranes, making the duct permeable so water flows out into the salty medulla. The result is a small volume of concentrated urine and conserved body water. When ADH is low, the duct stays watertight and the body produces large volumes of dilute urine.
8.2 The Renin–Angiotensin–Aldosterone System (RAAS)
This is the body’s master blood-pressure and sodium-conservation axis, and the kidney sits at its origin. When blood pressure or sodium delivery falls, specialised cells in the kidney (the juxtaglomerular apparatus) release the enzyme renin. Renin triggers a cascade: it converts angiotensinogen to angiotensin I, which is converted by ACE (mainly in the lungs) to angiotensin II — a potent vasoconstrictor that also stimulates the adrenal glands to release aldosterone.
- Angiotensin II constricts blood vessels (raising pressure) and promotes sodium reabsorption.
- Aldosterone acts on the collecting duct to reabsorb sodium (and water with it) while secreting potassium.
Why RAAS matters clinicallyBecause RAAS is so central to blood pressure, the most widely used blood-pressure medications — ACE inhibitors and angiotensin-receptor blockers (ARBs) — work by interrupting this very kidney-driven cascade.
8.3 Atrial Natriuretic Peptide (ANP)
ANP is the counterweight to RAAS. Released by the heart’s atria when they are stretched by high blood volume, it promotes the excretion of sodium and water, lowering volume and pressure — opposing the salt-retaining actions of aldosterone and angiotensin II.
9. The Kidney’s Endocrine and Metabolic Roles
Beyond regulating fluids, the kidney is a genuine endocrine organ, secreting hormones that influence tissues far beyond itself.
9.1 Erythropoietin and Red Blood Cell Production
Specialised cells in the kidney sense the oxygen content of the blood. When oxygen falls, they release erythropoietin (EPO), a hormone that travels to the bone marrow and stimulates the production of red blood cells. This is why chronic kidney disease so often causes anaemia: failing kidneys make too little EPO. It is also why EPO has been infamously abused as a performance-enhancing drug in endurance sport.
9.2 Activation of Vitamin D
Vitamin D from sunlight and diet is biologically inactive until the kidney performs the final activating step, converting it to calcitriol, the active form. Calcitriol is essential for absorbing calcium from the gut and maintaining healthy bones. Consequently, kidney failure frequently leads to bone disease and disturbed calcium balance — a condition known as renal osteodystrophy.
9.3 Gluconeogenesis and Blood Pressure
The kidney also contributes to glucose production during prolonged fasting (renal gluconeogenesis) and, through the RAAS and its control of fluid volume, serves as the dominant long-term regulator of blood pressure in the body. No other organ exerts comparable long-term control over arterial pressure.
Six jobs in one organFiltration of waste · electrolyte balance · acid–base regulation · blood pressure control · red blood cell stimulation · vitamin D activation. The breadth of these roles explains why kidney failure affects the entire body.
10. Acid–Base Balance
Human metabolism constantly generates acid, yet blood pH must stay within a razor-thin range of about 7.35 to 7.45. The lungs handle volatile acid by exhaling carbon dioxide, but the kidney is responsible for the slower, definitive regulation of fixed acid — and it is the only organ that can actually remove acid from the body and manufacture new buffer.
10.1 Reabsorbing Bicarbonate
Bicarbonate is the body’s principal buffer, and losing it in the urine would be disastrous. The proximal tubule reclaims essentially all filtered bicarbonate through an indirect mechanism: tubule cells secrete hydrogen ions that combine with filtered bicarbonate to form carbon dioxide and water (catalysed by carbonic anhydrase), which re-enter the cell and are reconverted to bicarbonate for return to the blood.
10.2 Generating New Bicarbonate and Excreting Acid
Reclaiming existing bicarbonate is not enough to offset daily acid production, so the kidney also makes new bicarbonate. It does this by excreting hydrogen ions bound to urinary buffers — chiefly phosphate (forming titratable acid) and ammonia (forming ammonium). For every hydrogen ion excreted this way, a fresh bicarbonate molecule is added to the blood. The kidney’s capacity to ramp up ammonia production is the main way it defends against a chronic acid load.
| Mechanism | Site | Effect on blood pH |
|---|---|---|
| Bicarbonate reabsorption | Proximal tubule | Prevents buffer loss |
| Titratable acid (phosphate) | Distal tubule | Excretes H⁺, adds HCO₃⁻ |
| Ammonium excretion | Proximal + collecting duct | Major adjustable acid removal |
11. The Juxtaglomerular Apparatus and Autoregulation
A recurring theme is the kidney’s ability to keep its own filtration steady despite swings in blood pressure. The control centre for this is the juxtaglomerular apparatus (JGA), a small structure where the distal tubule loops back to touch its own glomerulus.
The JGA contains macula densa cells that sense the salt concentration of the fluid passing through the distal tubule, and granular (juxtaglomerular) cells in the afferent arteriole wall that store and release renin. If filtration runs too fast, the macula densa detects the extra salt and signals the afferent arteriole to constrict, dialling filtration back down — a feedback loop known as tubuloglomerular feedback. Combined with a myogenic response in which arterioles automatically tighten when stretched by higher pressure, these mechanisms let the kidney hold GFR remarkably constant across a wide range of blood pressures.
Autoregulation in one sentenceThe kidney protects its own filtration rate through tubuloglomerular feedback and the myogenic response, keeping GFR stable even as systemic blood pressure rises and falls during ordinary daily life.
12. Nitrogenous Waste and What the Kidney Removes
The headline job of the kidney in popular understanding — removing waste — is real, even if it is only part of the story. The principal waste products cleared by the kidney are nitrogenous, arising from the breakdown of proteins and nucleic acids.
- Urea: the main nitrogenous waste, produced by the liver from ammonia generated during protein breakdown. It is also recycled to help concentrate urine.
- Creatinine: a by-product of muscle metabolism, filtered freely and barely reabsorbed — which makes its blood level a convenient marker of kidney function.
- Uric acid: from the breakdown of purines in nucleic acids; its accumulation can crystallise in joints, causing gout.
- Drugs, toxins, and excess ions: cleared by filtration and active secretion, which is why kidney function strongly affects drug dosing.
The kidney’s clearance of a substance — the volume of plasma cleared of it per minute — is the formal way physiologists quantify this removal, and the clearance of creatinine remains a practical estimate of overall kidney function.
13. When the System Fails: Clinical Correlations
The breadth of the kidney’s responsibilities means that its failure reverberates throughout the body. Examining disease illuminates function in reverse.
13.1 Acute Kidney Injury and Chronic Kidney Disease
Acute kidney injury (AKI) is a sudden, often reversible loss of function caused by, for example, severe dehydration, blood loss, toxins, or obstruction. Chronic kidney disease (CKD) is a progressive, usually irreversible loss of nephrons over months or years, most commonly driven by diabetes and high blood pressure. CKD is staged by GFR, and its advanced form requires dialysis or transplantation.
13.2 The Systemic Consequences of Failure
- Fluid overload and hypertension from impaired salt and water excretion.
- Hyperkalaemia and acidosis from failed potassium and acid handling.
- Anaemia from reduced erythropoietin.
- Bone disease from impaired vitamin D activation and disturbed calcium–phosphate balance.
- Uraemia — the build-up of nitrogenous waste, causing nausea, fatigue, and confusion.
13.3 Dialysis and Transplantation
Dialysis substitutes for the kidney’s filtering function by passing blood across an artificial membrane against a carefully formulated fluid, removing waste and excess water. Two main forms exist: haemodialysis, which circulates blood through an external machine several times a week, and peritoneal dialysis, which uses the patient’s own abdominal lining as the filtering membrane. But dialysis cannot replicate the kidney’s endocrine roles — it does not make erythropoietin or activate vitamin D — which is why transplantation, restoring a whole functioning organ, remains the superior long-term treatment.
| Function | Healthy kidney | Dialysis | Transplant |
|---|---|---|---|
| Waste filtration | Continuous | Intermittent | Continuous |
| Fluid removal | Precise | Approximate | Precise |
| Erythropoietin | Yes | No | Yes |
| Vitamin D activation | Yes | No | Yes |
| Blood pressure control | Yes | Partial | Yes |
The lesson of failureDialysis can replace filtration but not the kidney’s hormonal intelligence. This gap is the clearest proof that the kidney is far more than a filter.
14. Key Terms at a Glance
The following glossary consolidates the central terms used throughout this article for quick reference.
| Term | Meaning |
|---|---|
| Nephron | The microscopic functional unit of the kidney; ~1 million per kidney |
| Glomerulus | Capillary tuft where blood is filtered |
| Bowman’s capsule | Cup that captures the glomerular filtrate |
| GFR | Glomerular filtration rate; total volume filtered per minute |
| Loop of Henle | Hairpin tubule that builds the medullary concentration gradient |
| Reabsorption | Recovery of water and solutes from tubule back into blood |
| Secretion | Movement of substances from blood into the tubule for excretion |
| ADH | Antidiuretic hormone; controls collecting-duct water permeability |
| RAAS | Renin–angiotensin–aldosterone system; master blood-pressure axis |
| Aldosterone | Hormone that drives sodium retention and potassium secretion |
| Erythropoietin | Kidney hormone stimulating red blood cell production |
| Calcitriol | The active form of vitamin D produced by the kidney |
| GBM | Glomerular basement membrane; charged filtration layer |
| JGA | Juxtaglomerular apparatus; control centre for renin and autoregulation |
15. Conclusion: An Organ of Quiet Genius
The human kidney resists easy summary precisely because it does so much. It is a filter, but also a chemist, an endocrine gland, a blood-pressure regulator, and a guardian of the body’s internal chemistry. From the million nephrons working in parallel, to the molecular sieve of the slit diaphragm, to the elegant countercurrent geometry of the loop of Henle, the kidney achieves through structure what no single mechanism could accomplish alone.
What emerges from this analysis is a coherent picture: every structural feature serves a functional end, and every function ultimately serves a single overarching goal — homeostasis, the maintenance of a stable internal environment. The kidney does not merely respond to the body’s state; it actively defines the chemical conditions under which every other cell can survive. In filtering 180 litres a day to excrete barely one, in reclaiming exactly what is needed and discarding exactly what is not, in sensing oxygen and acid and pressure and responding with the right hormone at the right moment, the kidney embodies a kind of biological intelligence.
To understand the kidney, then, is to understand a central truth of physiology: that life is not the absence of change but the active, ceaseless work of holding the internal world steady against it. Few organs do that work more faithfully, or more quietly, than the pair of fist-sized filters tucked against the back of the abdomen.
In a single thoughtThe kidney is the organ that lets the rest of the body forget about chemistry — silently maintaining the precise internal conditions on which all other life processes depend.
The Human Kidney — Comprehensive Article, Essay & Analysis · Anatomy · Physiology · Biochemistry · Clinical Correlation

Be First to Comment